


引言
脑卒中分为出血性脑卒中和缺血性脑卒中(又称脑梗塞),其发病急骤、致死致残率高,是中国伤残调整生命年的第一大病因[1],其中脑梗塞的死亡率在我国各类疾病死亡原因中位居首位[2].中国国家卒中登记平台的数据显示,国内脑卒中患者第一年复发率为17.7%,5年的累积复发率>30%[3].随着医疗技术的进步和相关研究取得的进展,脑梗塞有了更好的治疗方案与治疗窗口,但其预后仍然不佳,尤其是中度和重度的患者.研究表明,脑血管疾病的复发率偏高,复发的致残危害程度高于首发;经过调研并随访相应病人,发现复发病人神经功能损伤明显加重[4].急性脑梗塞的复发给患者及家庭带来巨大的痛苦,同时给我国的医疗系统带来沉重的负担,因此,探讨急性脑梗塞患者复发影响因素的临床研究具有重要的临床意义.
1 资料与方法
1.1 研究对象
收集2013年9月至2022年8月在山东第二医科大学附属医院诊治的急性脑梗塞患者的临床资料和MR资料,所有患者均进行为期1年的随访.本研究已获我院伦理委员会批准(批准号wyfy-2023-kt-224). 复发性脑梗塞有多种定义[13-
图1
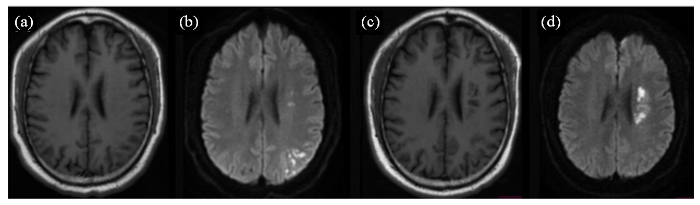
图1
一位多发急性脑梗塞复发患者磁共振轴位SE T1WI (a、c)、DWI (b、d)图像. 患者首次住院,行磁共振检查显示,左侧放射冠区和左侧顶叶区多个急性梗塞病灶,呈长T1信号(a),DWI弥散受限呈高信号(b);患者康复出院后6个月出现临床症状,行磁共振检查显示,左侧放射冠区多个急性梗塞病灶,呈长T1信号,左侧放射冠区见多个软化灶(c),DWI扩散受限呈高信号(d)
Fig. 1
Magnetic resonance axial SE T1WI (Fig. a, c) and DWI (Fig. b, d) of a patient with recurrent multiple acute cerebral infarcts. The patient was admitted to the hospital for the first time, and an MRI showed multiple acute infarction lesions in the left radiocaudate region and the left parietal lobe, with long T1 signals (Fig. a) and high DWI signals indicative of restricted diffusion (Fig. b). The patient developed clinical symptoms six months after discharge from rehabilitation, an MRI showed multiple acute infarction lesions in the left radiocaudate region with long T1 signals and multiple areas of infarction were also seen in the left radiocaudate region (Fig. c); diffusion-limited DWI with a high signal (Fig. d)
图2
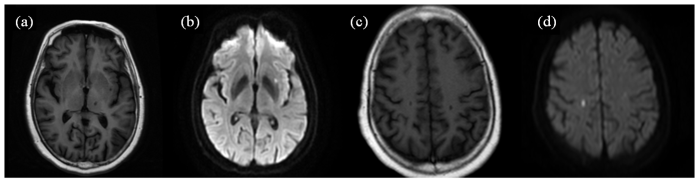
图2
一位单发急性脑梗塞复发患者磁共振轴位SE T1WI (a、c)、DWI (b、d)图像. 患者首次住院,行磁共振检查显示,左侧外囊单发腔梗呈长T1信号(a),DWI弥散受限呈高信号(b);患者康复出院后4个月出现临床症状,行磁共振检查显示,右侧顶叶单发腔梗灶,呈长T1信号(c),DWI扩散受限呈高信号(d)
Fig. 2
Magnetic resonance axial SE T1WI (Fig. a, c) and DWI (Fig. b, d) of a patient with recurrent single lesion of acute stroke.The patient was admitted to the hospital for the first time, and an MRI showed a single lumen infarction in the left external capsule with a long T1 signal (Fig. a) and diffusion-limited DWI with a high signal (Fig. b). The patient developed clinical symptoms four months after discharge from rehabilitation, an MRI showed a single lumen infarction in the right parietal lobe with a long T1 signal (Fig. c) and diffusion-limited DWI with a high signal (Fig. d)
1.2 磁共振检查和参数测量
磁共振检查采用Phillip Achieve 1.5 T超导磁共振成像仪器,使用8通道SENSE并行采集线圈.成像参数如下:轴位DWI序列(TR=3 000 ms、TE=75 ms、层厚6 mm、层间距1.5 mm,b值选择0、800 s/mm2);轴位SE T1WI序列(TR=500 ms、TE=20 ms、层厚6 mm、层间距1.5 mm).
研究表明,幕下小脑和脑干组织的供血主要源于椎基底动脉系统的各分支血管,而颈内动脉的各脑内分支血管供应相应的幕上脑组织[17].本研究中,定义主要脑动脉及其分支所灌注的脑组织范围为脑供血区. 其中,椎动脉分支含4个供血区:小脑后下动脉、小脑前下动脉、小脑上动脉和大脑后动脉.颈内动脉的主要脑内分支含4个供血区:后交通动脉分支、脉络膜前动脉、大脑前动脉和大脑中动脉.以此解剖概念作为基准,将以上各个血管的8个供血区域作为受累供血区的划分标准.
图3
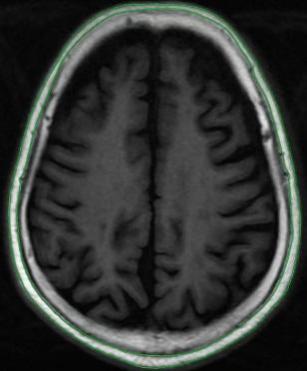
图3
磁共振轴位SE T1WI图像及头皮下脂肪区域勾画示意图
Fig. 3
Magnetic resonance axial SE T1WI image and a schematic diagram outlining the subcutaneous fat area
图4

图4
磁共振轴位SE T1WI图像(a)、DWI图像及病灶最大层面面积测量示意图(b). (a)中,左侧尾状核头部区急性梗塞病灶, 呈长T1信号;(b)中,DWI扩散受限呈高信号
Fig. 4
Magnetic resonance axial SE T1WI (a), DWI and the schematic diagram of the maximum lesion area measurement at the largest layer (b). In (a), MRI showed an acute infarction lesion in the head of the left caudate nucleus, presenting as long T1 signals; In (b), DWI showed restricted diffusion with high signal intensity.
1.3 统计学方法
测量数值均以均数±标准差(
2 结果与讨论
2.1 结果
表1 脑梗塞复发组和未复发组的一般资料比较
Table 1
| 相关因素 | 有无复发 | 统计值(χ²或Z) | p |
|---|---|---|---|
| 性别(χ²) | 有 | -0.178 | 0.239 |
| 无 | |||
| 年龄(Z) | 有 | 0.458 | 0.499 |
| 无 |
表2 脑梗塞复发组和未复发组的MRI数据的比较
Table 2
| 相关因素 | 有无复发 | 统计值(Z) | p |
|---|---|---|---|
| 病灶个数/个 | 有 | -3.611 | 0.000 |
| 无 | |||
| 受累供血区个数/个 | 有 | -2.997 | 0.003 |
| 无 | |||
| 所有病灶最大层面积/cm2 | 有 | -0.107 | 0.914 |
| 无 | |||
| 第四脑室上方层面头皮下 脂肪面积/cm2 | 有 | -0.411 | 0.681 |
| 无 |
2.2 讨论
本研究的两组患者间的性别、年龄无统计学的差异,排除以上条件干扰后,患者的磁共振影像表现可在一定程度上用于评估复发组和未复发组组间复发情况的差异.Xue等[8]的研究提示首发患者脑卒中的梗死灶面积与颈动脉的不稳定斑块的大小有关,梗塞灶越大,颈动脉含有不稳定和多发斑块的可能性越大,从而推断病人的复发率更大、预后更差.本研究测量了两组患者轴位图像上的病灶最大面积,但两组间的差异无统计学意义,提示病灶面积不是患者一年内是否复发的主要影响因素.有研究发现在头部脂肪沉积的情况下,异位脂肪分布可以作为评价肥胖患者代谢情况的一个重要指标[18].然而,本研究的结果显示,在急性脑梗塞患者的磁共振图像上,第四脑室上方层面头皮下脂肪面积在两组之间并没有显著的统计学差异.这意味着,在评价急性脑梗塞患者的预后时,患者磁共振图像上的头皮下脂肪面积并不是一个需要特别关注的指标.
本研究结果显示,急性脑梗塞复发组患者的病灶数量、受累供血区个数均多于未复发组,其差异有统计学意义.病灶数量、受累供血区个数影响复发的因素推测为以下三点.第一,更广泛的脑血管病变:病灶数量增多提示多支血管受累或弥漫性血管病变(如动脉粥样硬化、小血管病等),导致脑组织缺血范围更广;受累供血区增多反映多个血管床(如大脑中动脉、大脑前动脉、后循环等)同时或先后发生血流动力学障碍,提示整体脑血管储备功能下降[19].第二,更高的血栓负荷或栓塞风险:若为动脉-动脉栓塞(如颈动脉或心源性栓子),多发病灶可能反映栓子脱落更频繁或血管内皮损伤更严重[20];若为小血管病变(如腔隙性梗塞),多发病灶可能提示高血压、糖尿病等危险因素控制不佳,导致广泛小动脉硬化[21].第三,血流动力学代偿能力下降:多血管供血区受累可能意味着侧支循环代偿不足,使得患者在血压波动或低灌注时更易复发;Gupta等研究表明[22],当颈动脉狭窄严重并降低脑灌注压(cerebral perfusion pressure,CPP)时,脉管系统的自动调节将最大限度地扩张脑小动脉以维持脑血流(cerebral blood flow,CBF),随着CPP的进一步降低和小动脉的最大扩张,CBF也会降低并可能增加中风的风险.
尽管本研究揭示了病灶数量和受累供血区个数与急性脑梗塞复发的相关性,但仍存在以下局限性:本研究未进一步分析病灶分布模式(如分水岭区梗塞与穿支动脉梗塞)和分布数量(反映动脉粥样硬化血栓形成、心源性栓塞或小血管病变等不同机制)对于急性脑梗塞复发潜在的影响;同时未能结合血管影像(如管腔狭窄程度、斑块稳定性)进一步分析病灶分布模式与复发风险的关系来进一步验证脑梗塞的复发机制.本研究将进一步探究病灶数量/供血区个数与复发风险的量效关系,并且探讨这些特征与其他危险因素的交互作用,从而建立并验证其在临床风险评估模型中的价值.
3 结论
综上所述,对于本研究中的急性脑梗塞患者而言,性别和年龄并非其复发的相关因素,磁共振图像上的第四脑室上方层面头皮下脂肪面积、所有病灶最大层面积与其复发也没有相关性.本文数据表明,在MR-DWI图像上病灶个数和受累供血区个数是判断患者在一年内是否复发的重要因素,病灶个数和受累供血区个数可以反映出患者的缺血面积、侧支循环和血管再生能力等信息,从而进一步影响患者的预后.因此,对于急性脑梗塞患者,MR-DWI图像上的病灶个数和受累供血区个数可以为临床医师提供重要的影像学依据,帮助医生对患者进行个体化的治疗和预后评价.
利益冲突
无
参考文献
Brief report on stroke prevention and treatment in China, 2020
[J].
《中国脑卒中防治报告2020》概要
[J].
Loss of circadian rhythm of blood pressure following acute stroke
[J].Epidemiology of acute stroke in developing countries differs from that in the developed world, for example, the age at stroke, risk factors, subtypes of stroke and prognosis. Hypertension remains a dominant risk factor and prognostic indicator in patients with stroke in all communities. The risk of stroke is directly related to elevations of blood pressure. A number of clinical studies have shown that the control of hypertension leads to a reduction in the incidence of stroke in a community. However there is still considerable controversy surrounds the changes in blood pressure in various subtypes of strokes and problem of management of elevated BP after stroke. We studied the circadian rhythm of blood pressure in patients following acute stroke.To study the circadian rhythm of blood pressure, fifty consecutive patients with an acute stroke who were admitted to medical emergency within 120 hours of onset were included in the study. After a detailed history and clinical examination, a continuous blood pressure monitor (Spacelab 90207) was attached on the side ipsilateral to intracranial lesion (unaffected arm). The blood pressure was recorded for 24 hours at 15 minutes interval during daytime (6.00 am-6.00 pm) and 20 minutes interval overnight (6 pm to 6 am).Risk factors for stroke in 50 patients included hypertension in 31(62%), diabetes mellitus in 4 (8%), smoking in 13 (26%) and previous history of transient ischemic attack in 7 (14%) patients. Mean systolic pressure and diastolic pressure at admission were higher in patients with hemorrhagic stroke -29 patients (177 +/- 24 mmHg and 105 +/- 19 mmHg respectively) compared to patients with ischemic strokes-21 patients (150 +/- 36 mm Hg and 89 +/- 18 mm Hg respectively, p value <0.01 in both comparisons). The normal diurnal variation in blood pressure (night time dipping of more than 10%) was abolished in 44 (88%) of patients. Out of 44 nondippers, 29 patients showed reverse dipping i.e. rise of BP during night time compared to day time levels. None of the risk factors, clinical or laboratory variables, type of stroke or blood pressure changes differed significantly between these two groups.Therefore, we showed a pathologically reduced or abolished circadian BP variation after stroke. Absence of normal dipping results in a higher 24 hour blood pressure load and may have more target organ damage than those with normal diurnal variation of blood pressure.
Interpretation on the report of global stroke data 2022
[J].
解读2022年全球脑卒中数据报告
[J].
Research progress on risk factors of recurrent cerebral infarction
[J].
复发性脑梗死危险因素的研究进展
[J].
Persistence and adherence to secondary preventive medication in ischemic stroke patients and its influence on prognosis
[J].
缺血性脑卒中后二级预防药物依从性现状及对预后的影响
[J].
Influencing factors analysis of recurrence in acute ischemic stroke based on propensity score matching
[J].
基于倾向性评分匹配法的急性缺血性脑卒中患者复发的影响因素分析
[J].
Mortality and recurrent vascular events after first incident stroke: a 9-year community-based study of 0.5 million Chinese adults
[J].DOI:10.1016/S2214-109X(20)30069-3 URL [本文引用: 1]
Relationship between infarct area and plasma fibrinogen level with carotid plaque in recurrent cerebral infarction patients
[J].
复发性脑梗死病人梗死灶面积与血浆纤维蛋白原水平、颈动脉斑块的关系研究
[J].
Brain age assessment of patients with major depressive disorder based on convolutional neural network
[J].
基于卷积神经网络的重度抑郁症患者大脑年龄评估
[J].
DOI:10.11938/cjmr20233081
[本文引用: 1]

大脑年龄已成为神经退行性疾病诊断和机理研究的重要分析对象. 重度抑郁症是否会增加患者的大脑年龄,尚未得到一致的结论,且该方向的研究在中国人口内开展较少. 本文使用从中国25家医院收集的REST-meta-MDD数据集,构建基于高分辨率T1-加权3D大脑结构磁共振图像的卷积神经网络模型,用于预测患者的大脑年龄,计算与实际年龄的差异. 最终结果的平均绝对误差和相关系数为3.16和0.93,与健康组对比,重度抑郁症患者的平均大脑年龄增加了3.94年,进一步确认了重度抑郁症会加速大脑衰老,且患病程度与患者的性别、年龄和受教育程度相关. 对比传统机器学习算法,该模型取得结果的平均绝对误差更小,相关系数更高.
Evaluation of the impact of b-value ranges on six body diffusion models in prostate application
[J].
b值范围对6种体部扩散模型在前列腺应用的影响评估
[J].论文研究了不同b值采集范围对6种体部扩散模型定量参数计算的影响.研究涉及扩散模型包含单指数模型(Mono)、扩散峰度成像(DKI)、体素内非相干运动模型(IVIM)、扩散拉伸指数模型(SEM)、分数微积分模型(FROC)和随机游走模型(CTRW),b值范围0~2 500 s/mm<sup>2</sup>.通过扩散模型参数之间的相关性、t检验以及前列腺病灶良恶性鉴别能力三个维度,评估了不同b值采集范围对参数计算的影响.结果显示与参考采样方案相比,随着最大b值降低,所得同一扩散参数感兴趣区域(ROI)均值的差异逐渐增大,但相关性降低不明显,且前列腺病灶良恶性的鉴别能力也保持相似水平.基于实验结果,建议在临床实践中采用b值范围为0~1 500 s/mm<sup>2</sup>的采集方案.这一方案在具备较高采集效率的同时,一半以上参数与参考采样方案结果的相关性不低于0.98,且良恶性鉴别能力指标曲线下面积(AUC)值的差别小于0.01.此外,不同扩散模型对于b值方案的敏感性存在差异,其中SEM和CTRW模型的参数受b值范围的影响相对较小.
Rapid imaging of pulmonary ventilation function evaluation with 129Xe MRI
[J].
Diffusion-and perfusion-weighted MRI: The DWI/PWI mismatch region in acute stroke
[J].
DOI:10.1161/01.STR.30.8.1591
URL
[本文引用: 1]
\n Background and Purpose\n —Diffusion-weighted imaging (DWI) and perfusion-weighted imaging (PWI) are relatively new MR techniques increasingly used in acute stroke. During the first hours of stroke evolution, the regions with abnormal perfusion are typically larger than the DWI lesions, and this mismatch region has been suggested to be “tissue at risk.” The aim of this study was to evaluate the PWI/DWI mismatch region in acute stroke patients and find parameters indicative of both infarct progression and functional impairment.\n
Early risk of recurrence by subtype of ischemic stroke in population-based incidence studies
[J].
DOI:10.1212/01.wnl.0000110311.09970.83
PMID:14981172
[本文引用: 1]
To study the early risk of recurrent stroke by etiologic subtype.The authors studied risk of recurrent stroke by etiologic subtype (Trial of ORG 10172 in Acute Stroke Treatment [TOAST] classification) in patients in two population-based studies: the Oxford Vascular Study and the Oxfordshire Community Stroke Project. A meta-analysis was performed with data from the only two other published studies reporting equivalent data.The four studies included 1,709 strokes with 30 recurrences at 7 days, 72 at 30 days, and 113 at 3 months. Recurrent stroke risk varied between subtypes (p < 0.001). Compared with other subtypes, patients with stroke due to large-artery atherosclerosis (LAA) had the highest odds of recurrence at 7 days (odds ratio [OR] = 3.3, 95% CI = 1.5 to 7.0), 30 days (OR = 2.9, 95% CI = 1.7 to 4.9), and 3 months (OR = 2.9, 95% CI = 1.9 to 4.5). Odds of recurrence at 30 days for other subtypes were cardioembolic (OR = 1.0, 95% CI = 0.6 to 1.7), undetermined (OR = 1.0, 95% CI = 0.6 to 1.6), and small-vessel stroke (OR = 0.2, 95% CI = 0.1 to 0.6). There was no significant heterogeneity between the studies. Although only 14% of strokes were associated with LAA, this subtype accounted for 37% of recurrences within 7 days.The risk of early recurrent stroke is highest in patients with LAA. This supports the need for urgent carotid imaging and prompt endarterectomy.
The WHO STEP wise approach to stroke surveillance
[J].
Plasma tissue kallikrein level is negatively associated with incident and recurrent stroke: a multicenter case-control study in China
[J].
DOI:10.1002/ana.22404
PMID:21823154
[本文引用: 1]
Tissue kallikrein (TK) cleaves kininogen to produce the potent bioactive compounds kinin and bradykinin, which lower blood pressure and protect the heart, kidneys, and blood vessels. Reduction in TK levels is associated with cardiovascular disease and diabetes in animal models. In this study, we investigated the association of TK levels with event-free survival over 5 years in Chinese first-ever stroke patients.We conducted a case-control study with 1,268 stroke patients (941 cerebral infarction, 327 cerebral hemorrhage) and 1,210 controls. Plasma TK levels were measured with an enzyme-linked immunosorbent assay. We used logistic regression and Cox proportional hazards models to assess the relationship between TK levels and risk of first-time or recurrent stroke.Plasma TK levels were significantly lower in stroke patients (0.163 ± 0.064mg/l vs 0.252 ± 0.093mg/l, p < 0.001), especially those with ischemic stroke. After adjustment for traditional risk factors, plasma TK levels were negatively associated with the risk of first-ever stroke (odds ratio [OR], 0.344; 95% confidence interval [CI], 0.30-0.389; p < 0.001) and stroke recurrence and positively associated with event-free survival during 5 years of follow-up (relative risk, 0.82; 95% CI, 0.74-0.90; p < 0.001). Compared with the first quartile of plasma TK levels, the ORs for first-ever stroke patients were as follows: second quartile, 0.77 (95% CI, 0.56-1.07); third quartile, 0.23 (95% CI, 0.17-0.32); fourth quartile, 0.04 (95% CI, 0.03-0.06).Lower plasma TK levels are independently associated with first-ever stroke and are an independent predictor of recurrence after an initial stroke.Copyright © 2011 American Neurological Association.
Chinese Guidelines for diagnosis and treatment of acute ischemic stroke 2023
[J].
中国急性缺血性卒中诊治指南2023
[J].
Study of relation between MRI findings of infratentorial metastasis of lung cancer and its blood distribution
[J].
肺癌幕上脑转移瘤与血供关系的MRI研究
[J].
Correlation between head fat and metabolism in patients of obesity
[J].
肥胖患者头部脂肪与代谢的相关性
[J].
MRI-visible perivascular spaces in cerebral amyloid angiopathy and hypertensive arteriopathy
[J].
DOI:10.1212/WNL.0000000000003746
PMID:28228568
[本文引用: 1]
To assess MRI-visible enlarged perivascular spaces (EPVS) burden and different topographical patterns (in the centrum semiovale [CSO] and basal ganglia [BG]) in 2 common microangiopathies: cerebral amyloid angiopathy (CAA) and hypertensive arteriopathy (HA).Consecutive patients with spontaneous intracerebral hemorrhage (ICH) from a prospective MRI cohort were included. Small vessel disease MRI markers, including cerebral microbleeds (CMBs), cortical superficial siderosis (cSS), and white matter hyperintensities (WMH), were rated. CSO-EPVS/BG-EPVS were assessed on a validated 4-point visual rating scale (0 = no EPVS, 1 = <10, 2 = 11-20, 3 = 21-40, and 4 = >40 EPVS). We tested associations of predefined high-degree (score >2) CSO-EPVS and BG-EPVS with other MRI markers in multivariable logistic regression. We subsequently evaluated associations with CSO-EPVS predominance (i.e., CSO-EPVS > BG-EPVS) and BG-EPVS predominance pattern (i.e., BG-EPVS > CSO-EPVS) in adjusted multinomial logistic regression (reference group, BG-EPVS = CSO-EPVS).We included 315 patients with CAA-ICH and 137 with HA-ICH. High-degree CSO-EPVS prevalence was greater in CAA-related ICH vs HA-related ICH (43.8% vs 17.5%, < 0.001). In multivariable logistic regression, high-degree CSO-EPVS was associated with lobar CMB (odds ratio [OR] 1.33, 95% confidence interval [CI] 1.10-1.61, = 0.003) and cSS (OR 2.08, 95% CI 1.30-3.32, = 0.002). Deep CMBs (OR 2.85, 95% CI 1.75-4.64, < 0.0001) and higher WMH volume (OR 1.02, 95% CI 1.01-1.04, = 0.010) were predictors of high-degree BG-EPVS. A CSO-EPVS-predominant pattern was more common in CAA-ICH than in HA-ICH (75.9% vs 39.4%, respectively, < 0.0001). CSO-PVS predominance was associated with lobar CMB burden and cSS, while BG-EPVS predominance was associated with HA-ICH and WMH volumes.Different patterns of MRI-visible EPVS provide insights into the dominant underlying microangiopathy type in patients with spontaneous ICH.© 2017 American Academy of Neurology.
Significance of acute multiple brain infarction on diffusion-weighted imaging
[J].
DOI:10.1161/01.str.31.3.688
PMID:10700505
[本文引用: 1]
Diffusion-weighted imaging (DWI) is superior to conventional MRI in identification of small new ischemic lesions and discrimination of recent infarcts from old ones. Thus, this technique is useful in the detection of acute multiple brain infarcts (AMBI). We sought to determine the frequency and the topographical and etiologic patterns of AMBI detected on DWI.We studied 329 consecutive ischemic stroke patients who underwent DWI and MRI/MR angiography within 4 days of stroke onset. AMBI was defined as noncontiguous high signal intensities on DWI in >1 vascular territory. Stroke mechanism was determined according to the criteria of the Trial of Org 10172 in Acute Stroke Treatment (TOAST).We detected AMBI in 95 patients (28.9%). AMBI in anterior circulation was found in 62 cases: in 1 hemisphere in 42 (group A) and in bilateral hemispheres in 20 (group B). Twenty-two patients had AMBI in the posterior circulation (group C) and 11 in both anterior and posterior circulations (group D). The most frequent cause of stroke was large-artery atherosclerosis in groups A (33/42), B (9/20), and C (15/22) (P=0.02) and cardioembolism in group D (6/11) (P=0.02). Elevated fibrinogen or hematocrit was significantly associated with group B (P=0.01). In 9 patients in groups B and D, anatomic variations of anterior or posterior cerebral arteries or patent posterior communicating artery contributed to AMBI.Different topographical patterns of AMBI are associated with different vascular pathologies and stroke mechanisms. Hemorheologic abnormality or vascular anatomic variations may be contributing factors in the pathogenesis of AMBI in bilateral cerebral hemispheres or in both anterior and posterior circulations.
Small vessel disease: mechanisms and clinical implications
[J].
DOI:S1474-4422(19)30079-1
PMID:31097385
[本文引用: 1]
Small vessel disease is a disorder of cerebral microvessels that causes white matter hyperintensities and several other common abnormalities (eg, recent small subcortical infarcts and lacunes) seen on brain imaging. Despite being a common cause of stroke and vascular dementia, the underlying pathogenesis is poorly understood. Research in humans has identified several manifestations of cerebral microvessel endothelial dysfunction including blood-brain barrier dysfunction, impaired vasodilation, vessel stiffening, dysfunctional blood flow and interstitial fluid drainage, white matter rarefaction, ischaemia, inflammation, myelin damage, and secondary neurodegeneration. These brain abnormalities are more dynamic and widespread than previously thought. Relationships between lesions and symptoms are highly variable but poorly understood. Major challenges are the determination of which vascular dysfunctions are most important in pathogenesis, which abnormalities are reversible, and why lesion progression and symptomatology are so variable. This knowledge will help to identify potential targets for intervention and improve risk prediction for individuals with small vessel disease.Copyright © 2019 Elsevier Ltd. All rights reserved.
Cerebrovascular reserve and stroke risk in patients with carotid stenosis or occlusion: a systematic review and meta-analysis
[J].
DOI:10.1161/STROKEAHA.112.663716
PMID:23091119
[本文引用: 1]
Impairments in cerebrovascular reserve (CVR) have been variably associated with increased risk of ischemic events and may stratify stroke risk in patients with high-grade internal carotid artery stenosis or occlusion. The purpose of this study is to perform a systematic review and meta-analysis to summarize the association of CVR impairment and stroke risk.We performed a literature search evaluating the association of impairments in CVR with future stroke or transient ischemic attack in patients with high-grade internal carotid artery stenosis or occlusion. We included studies with a minimum of 1-year patient follow-up with baseline CVR measures performed by any modality and primary outcome measures of stroke and/or transient ischemic attack. A meta-analysis with assessment of study heterogeneity and publication bias was performed. Results were presented in a forest plot and summarized using a random-effects model.Thirteen studies met the inclusion criteria, representing a total of 1061 independent CVR tests in 991 unique patients with a mean follow-up of 32.7 months. We found a significant positive relationship between impairment of CVR and development of stroke with a pooled random effects OR of 3.86 (95% CI, 1.99-7.48). Subset analysis showed that this association between CVR impairment and future risk of stroke/transient ischemic attack remained significant regardless of ischemic outcome measure, symptomatic or asymptomatic disease, stenosis or occlusion, or CVR testing method.CVR impairment is strongly associated with increased risk of ischemic events in carotid stenosis or occlusion and may be useful for stroke risk stratification.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}